MIM(Prisons) is a cell of revolutionaries serving the oppressed masses inside U.$. prisons, guided by the communist ideology of Marxism-Leninism-Maoism.
Under Lock & Key is a news service written by and for prisoners with a focus on what is going on behind bars throughout the United States. Under Lock & Key is available to U.S. prisoners for free through MIM(Prisons)'s Free Political Literature to Prisoners Program, by writing:
MIM(Prisons) PO Box 40799 San Francisco, CA 94140.
At the moment, during this pandemic and major outbreak inside
prisons, CDCR has decided that it is best to shuffle/transfer prisoners
like never before in prison history. There are transfers going on, on a
major scale, daily. The administration sent out a memo and order to open
up a ‘quarantine’ block in every prison across California designated for
people coming in from and going to another prison –- we are being
quarantined for fourteen days on our way in and out, at every stop.
Before, if you’d asked any prisoner in California if they ever got
transferred out a prison they didn’t wanna be in or got transferred due
to their custody points level dropping (therefore belonging to a
lower/higher security yard) they would answer ‘fuck no’!!! People would
be stuck in a Level 4 yard (high security) while being Level 3 (lower
security) eligible for up to years at a time – or at the very least, six
months. And now, at this precise moment and time of outbreak and
pandemic, CDCR decides to look at each case factor and execute transfers
according to their ‘code.’ People are coming in and out of every prison
in California to these designated ‘quarantine blocks.’ For the first
time ever, Level 1, 2, 3 and 4 are meeting up in these blocks, meeting
up from all prisons and transferring out to all prisons. It would be
irresponsible to think that this is not an operation by the system with
the intent and agenda to exterminate its population.
On paper, the administration is making it look good by conducting and
documenting daily medical and temperature checks for the two weeks of
quarantine, and doing two COVID-19 swab tests before allowing prisoners
on a transportation bus… but what CDCR is not telling the
public is that if one refuses to take a temperature check and refuses to
take the COVID-19 swab test, you will still be transferred, still get on
the bus, still spread whatever you have around, still use the same
showers, phone, water fountain, and be allowed to roam around!!! Yes,
the ones that refuse do not leave on the 14th day mark, instead they’re
documented as not transferring due to their refusal, etc. But CDCR still
transfers them after an additional week of being on ‘quarantine.’ In the
fifteen years I’ve been captive, never have I ever seen so many
transfers myself –- nor seen the prison system shuffled up in this
manner where we have about 10-15 prisons in one ‘block.’ We got people
from Chino, Folsom, Lancaster, Jamestown, Corcoran, Salinas, Delano, San
Quentin, Calipatria, the Bay, Solano, High Desert, all coming in four
times a week on a consistent basis, and we are all confined in these
newly implemented ‘quarantine blocks.’ How’s this for fighting
COVID-19?
One would be ignorant not to see what these suits and ties at the
table are putting in motion here. I’ve been doing my research and
talking to people as they come from all these prisons they are coming
from and it is amazing to hear how correctional officers and wardens are
bouncing people around within the prison itself before shipping
them out, how the administration gave out orders to correctional
officers to do this, do that, try this under the ruse of combating
COVID-19 while putting prisoners in harm’s way via reckless transfers.
The stories are lengthy and too many to describe, but I will do so in a
future piece and with proper equipment. For now, I’ll just use my case
and experience as a small window to provide insight to the public about
what the system is doing and to expose their agenda.
First off, I am a radikal intellectual, politikal prisoner, activist,
abolitionist, revolutionary, Sureno artist, who has been targeted by the
system throughout the years and well-documented. I was housed at New
Folsom for three years before the pandemic kicked off and I went under
quarantine. I had just got out the hole because the administration
attempted to blame and charge me for an attempted murder that I had no
knowledge of. I was back on the main line after the long battle of the
torture and mental stress of being in the hole, then out of nowhere, the
administration kidnaps me once again and I’m placed under another
‘investigation.’ They refused me my due process of signing a liability
chrono to go back to the yard, and instead stuffed me in the hole
again.
Then, as COVID-19 begins to worsen inside the prison, the
administration puts me on a bus … I end up in Lancaster … I’m there for
two weeks, then they let me run around the prison for one full day just
to come back to my living quarters to be informed that I’m gonna be
transferred again!!! I’m like, what the fuck is going on here? I’m
telling the counselor, captain, committee, that what they are doing is
wrong and how they putting me and everyone else at greater risk of
getting sick by doing this. They told me that is not them, its the
federal courts who ordered this!! I’m trying to tell them about all
they’re doing wrong and how I just got to that prison two weeks prior
that, etc. … nope, nothing, on another bus!! Now I get to Calipatria and
I come to find out that everyone around me is experiencing the same
thing! I was already in a yard of my ‘custody level’ so why continue to
shuffle people like there’s no tomorrow? It is clear to see what’s
happening here. If there’s a way I can file a lawsuit or join one
already taking place I would like to do that. If not, well fuck it, its
still fuck CDCR on mine!! Nothing about what this system is attempting
to do is towards a healthy California – the only ones making sure we
maintain a healthy structure is the prisoners ourselves and our loved
ones. The agenda of the system is still more boxes and forms of
genocide, war, population control.
On 15 June 2020, swab tests for COVID-19 were performed outside East
Block on what is called G yard. Donner’s 1st tier and 2nd tier (now
occupied by a group of grade B condemned prisoners from the AC which is
being used as a quarantine unit) are now waiting to see who got infected
by the disrespectful sows too righteous in their own eyes to cover their
snouts.
Since 29 May 2020 forward, less and less care is being seen. Trays
went from having no lids to being paper without much if anything
protecting them from any number of pathogens during food seizure.
On the morning of 15 June 2020 and throughout early afternoon,
locking cuff ports were installed on holding cages. When asked why no
plexiglass partitions were installed (because the cages are literally
only separated by the grated walls they’re made of) the installer’s
response was “they’re doing a lot of stupid things right now.” That
rings truer than wanted.
New rules implemented 1 June 2020 got rid of CDCR 22 forms. The
purpose of such forms was, according to DOM54.090.1 policy, to document
communication between staff and inmates. By getting rid of a way to
document communication between staff and inmates it opens up a trap door
for things like grievances to fall through. It also shuts down any
prisoner’s attempt to resolve problems in a timely manner that could and
now will spin out into oblivion. Of course, CDCR must have another
purpose for invoking “emergency regulations” as regards the appeals
process (see 15 CCR 3084-3086 on
http://www.cdcr.ca.gov/regulations/adult_operations). But CDCR hasn’t
said what the emergency is concerning appeals and/or CDCR 22 forms. Why
not emergency enforcement of 15 CCR 3052(e)(f)? Why not emergency
training for disrespectful sows that don’t tuck their snouts into their
masks?
On 16 June 2020 Donner condemned is allowed yard with 1/2 of East
Block (one day after testing and before results). It turns out EB is
getting fed with normal trays that have lids. When confronted, staff
explained that it’s because the kitchen doesn’t want to chance spreading
COVID-19. Nobody in Donner has tested positive, but 2 prisoners with
“symptoms” were moved to the AC. Even still, how does serving food
uncovered on a paper tray stop the spread of anything? The bullshit
thickens.
On 22 June 2020, ABC News at 5 did a story called “Outbreak at San
Quentin”. It did have snippets of testimony and video footage but it was
edited to be misleading. It casts CDCR as being proactive and without
cases until a transfer of inmates from Chino. Not only is that bullshit,
it explains nothing about how death row prisoners became infected having
no contact with those Chino prisoners. As of 15 June 2020, at least 30
of the other 300 reported infected prisoners at San Quentin are death
row prisoners currently warehoused in Donner Section.
The virus will continue to spread out of control because of staff’s
extreme lack of care expressed by their actions and/or reckless
disregard for the health & safety of both themselves and others.
Today (23 June 2020) two of the disrespectful sows assigned to Donner
RC (Busseman and Peters) began their daily asinine antics by first
prepping the RC prisoner food without face coverings. Later, the same
two handled the 5th tier’s canteen without face coverings or gloves.
Then they handed it to each of the intended recipients. Prisoners
continue to be put at risk when exposure is available. This outbreak
springs from an extreme lack of care NOT Chino.
According to the news ticker going across the bottom of the TV
screen, KPIX 5 reports over 160 death row prisoners have tested positive
for COVID-19 (as of 26 June 2020). More than 1/4 of all DR prisoners! In
addition to not wearing their masks properly or not at all, the
disrespectful sows assigned to Donner continue to follow orders to do
other really stupid things which facilitate the spread of the virus.
Death row prisoners warehoused in Donner take showers in cages with no
way to be more than 3’ from the prisoner in the cage next to them.
Here’s another example of stupid from the guy who built them. When
drunkard Ron Denis was warden at S.Q. he decided to prohibit prisoners
from using the yard showers. Rumor has it that the decision was in
response to female employees complaining about seeing naked men. A
stenciled sign was also posted on each yard prohibiting “bathing”. That
reactionary mole only detracts from what would be an available option.
Death row prisoners have been denied yard for 12 days as of 28 June
2020. However, a continuing lack of care blinds the S.Q.
administration’s ability to see and implement common sense solutions.
The present plan seems to be keep everyone locked in the units (health
professions warned have such poor ventilation) until all prisoners are
eventually exposed to a lethal dose of bullshit. Appeal #SQ-A-20-01123
recently submitted 29 March 2020 was due 29 June 2020 but continues to
be ignored despite the issues cited therein being major contributing
factors to the spread of COVID-19.
According to KPIX News (30 June 2020) a 71-year-old man on the row
died in his cell last week from COVID-19. CDCR is now assigning blame to
outside hospitals to further bury the fact its own employees NOT wearing
face coverings correctly or not at all are willing accessories.
The same report mentions 40 prisoners have been transferred to an
outside hospital due to COVID. Stepping up enforcement of Newsom’s mask
mandate has been and remains a joke as “essential employees” such as
Busseman, Peters, Alwhart, Costa and others “on assignment” for now or
who returned after being infected themselves remain a vector refusing to
properly wear or wear a face covering at all. Unfortunately, it is that
same selfish attitude that has led to the sharp spike in this whole
state - this whole country. According to every employee asked who
returned after a bout with the virus, S.Q. is NOT testing for the virus
prior to their return. These employees explained all S.Q. did was basic
symptom checks without any requirement to actually test negative for
COVID-19.
Now that CDCR says all its employees at S.Q. have been tested it
seems as if quite a few of those employees think a negative test means
you’ll never get COVID-19. But they could now get it (or give it)
walking into any cell block. Here’s another illustration to help make
this point more clear: on 15 June 2020 all death row prisoners being
warehoused in Donner Section were swab tested for COVID-19. Those who
tested positive could have been infected 2 weeks or more before the test
was done - BEFORE the transfer of prisoners from Chino even arrived.
Those who tested negative could have been infected while en route back
to their cell under “hands on escort” AFTER being tested.
On 1 July 2020 Gov. Newsom said nothing about the skyrocketing cases
of COVID-19 at S.Q. “Technical difficulties” prevented any questions
from the media. The Gov. went on about contact tracing for a moment but
the narrative surrounding the cause of the outbreak here remains
fictionalized in the mainstream version of events.
On the same day, later that evening it was put out on the wire that
another death row prisoner died. From what remains undisclosed at this
time. Can Gov. Newsom put a moratorium on the Pestilence Pilot
Program?
So like so many Californians I watched the governor’s speech.
Sitting in my 8x10 cell I watched yesterday as Governor Newsom spoke on
the impact of COVID-19. The spiking of coronavirus in our state and the
prison outbreak in California.
He spoke about coming out to Vacaville the day before to oversee the
building of a tent city out on the yard. His project is meant to reduce
the population of San Quentin State Prison due to out break of
coronavirus and all the deaths there by moving them out. Implying the
truth with out coming straight out and saying it, that they would move
them here. Thereby, jeopardizing an already medically fragile community
housed here at CMF, which is in fact a hospital. Most of us here are 55+
years of age with medical issues, many of which are the underlying
medical conditions we hear them referring to all the time when
discussing the COVID-19 pandemic. I wonder, is this the Governor’s plan
to reduce the population of CDCR?
But reducing the population of CDCR by means of population control
by euthanization through coronavirus?
They are expecting the virus to spread like wild fire here, now like
it did at San Quentin. Even more so because of the medically fragile
population here.
But when it does, don’t believe the lies and fairy tales that CDCR
will put out on it, and Governor Newsom stories of caring about
incarcerated populations. Because his actions prove otherwise.
MIM(Prisons) adds: One persyn recently told eir story
of being released from San Quentin prison and dropped off at the San
Rafael transit center, as is standard practice. After riding a bus to
San Francisco, this persyn got off the bus with flu-like symptoms and
passed out on a bench. Ey tested positive for COVID-19 immediately after
release.(Snap Judgement on National Public Radio, 25 July 2020)
California, which began the pandemic as the good example in the
United $tates, is quickly going downhill as capitalism demands business
opens up to “keep the economy going.” Meanwhile, the San Quentin
humanitarian disaster is an embarrassment for the CDCR across the
country and in the global news. Yet, the staff still seem proud to
violate safety procedures and endanger the people around them.
The sickness that is spreading throughout the population of the
United $tates that is due to the COVID-19 virus is just a symptom of a
deeper sickness that is the individualism and cruel sadism that has
allowed the virus to spread so much more in this country than in others.
It is no coincidence that this cowboy, settler, #1 imperialist country
in the world sees itself as superior and invincible and enjoys
inflicting suffering on others. These characteristics are required to
keep imperialism going. Yet, this pandemic is an example of how these
characteristics will be part of this empire’s undoing. They are
intentionally spreading a disease among their own people, even as the
oppressed and the imprisoned suffer disproportionately from their
behavior. Recent events have only strengthened the oppressed peoples’
cries for organized resistance that serves humyn need. It is in these
conditions that real leaders and servants of the people must act to
bring us to a new stage of history.
Greetings, I am writing in hopes you may be able to help and/or
advise me. It is my intention to file suit against the Texas Department
of Criminal Justice (TDCJ) director and employees concerning TDCJ
failure to address grievance issues such as:
Denial of insulin to insulin dependent diabetic
Transport Officer Mr. Ballew stated in the court hearing on 30
January 2019 that I must provide my own insulin during transport. I
filed grievance #9019034096 on 6 February 2019 concerning this issue and
unit grievance office claims to have closed this grievance on 1 January
2019. I must pay for a copy if I want to see the response given. (How is
it possible to close grievance before it’s filed?)
When I was released from the UTMB hospital and transferred to this
(the Terrell Unit) I requested my property from the Carole Young
infirmary unit be sent to me. I was told it was sent to the Byrd Unit
and to date I have not received any property from the Byrd or Carole
Young Units and my grievances step two, dated 12 April 2019, has been
completely forged including the signing of my name to the document as if
I wrote it.
It is my intentions to bring suit under violation of government code
S.504 rehabilitation act for the following reasons:
I am denied to participate in TDCJ and UTMB programs and services or
the benefit of those services provided to all other prisoners.
UTMB Galveston hospital orders that I take insulin three times a day.
Note: I am not a type one or type two diabetic. I do not have a pancreas
after it was surgically removed leaving me a severe diabetic with an
auto-immune deficiency. My life depends on insulin and when I am not
receiving insulin as ordered I am denied the right to complain through
the TDCJ grievance program.
I request you send me the additional resource application to the
federal courts and a copy of TDCJ grievance codes manual and any
additional advice or information you may provide will be helpful. Also
know that I talked with the Terrell Unit Assistant Warden Mr. Antony
Patrict about these issues and he said “Sue me!” And the grievance
office refused to allow me to complain about the forged grievance from
12 April 2019.
I want to provide y’all with an attorney’s address that is seeking to
help Texas prisoners who have been denied dentures, further causing
irreversible damages, as well as pain and suffering.
Contact them directly: Randall Kallinen 511 Broadway St.
Houston, TX 77027
I know he’s putting together a class action suit. I don’t know if
there’s a deadline in contacting him or if he’s only able to accept so
many people, but if y’all can help bring awareness to Texas comrades I’d
be very appreciative.
MIM(Prisons) adds: In September 2018 the Houston Chronicle
broke a story about TDCJ denying prisoners dentures, and telling them to
eat pureed food instead. In December 2018, it was reported that TDCJ
will begin using 3D printers to make dentures for prisoners. We’re not
sure about the status of this class action suit, but we encourage
readers who fall in this class to contact Attorney Kallinen directly.
While not directly related to our mission of ending oppression through
the complete overthrow of the capitalist economic system, standing up
for our humyn dignity in our present moment helps give us more strength
to take on such a poweful enemy.
MIM(Prisons) distributes a number of resources for activists in Texas
prisons. We ask for donations to cover the cost to print and mail the
materials. We can accept donations in stamps or money orders.
Texas Campaign Pack - $3.50 Sworn Complaint Form - SASE or 2
stamps PD-22 Codes - $5 TDCJ Grievance Manual - $10 (These
materials are also available for free online.)
We heard that TDCJ is changing its practice on the grievance manual and
will start stocking it in the prison law library. Please send
confirmation on this if you know!
The prison’s segregation unit at Calhoun State Prison (CSP) has a
practical policy of delaying an insulin-dependent diabetic’s
finger-stick & insulin injection until several hours after meals
have already been served and the empty meal trays collected back up.
This is even though their medical orders call for them to receive
finger-sticks & insulin before meals, not afterward. This is a
textbook example (or, in this prison setting, a case-law example) of a
prison policy of indifference which exists in violation of both the
contemporary standards recognized by the medical profession (medical
malpractice), and the federal constitution’s 8th Amendment’s
proscription against cruel & unusual punishments.
A factor contributing to this policy is that at CSP’s segregation (seg)
unit breakfast is passed out anytime between 4:30 a.m. & 5 a.m. but
CSP’s administration doesn’t have its medical staff clocking in for work
until 6 a.m. every morning. By that time (1-1.5 hours after breakfast)
the diabetics housed in seg are badly in need of relief from the
dangerously high blood glucose/sugar level resulting from their having
ate breakfast without any insulin. I know from my own experience as an
insulin-dependent diabetic that if I eat without first taking insulin I
develop a dangerously high glucose level in the 300s, 400s, 500s, or
higher. This is a typical insulin-dependent’s reaction to eating without
first receiving the prescribed dosage of insulin he requires for the
particular meal.
When nurses clock in at 6 a.m. all of the diabetics housed in prison
general population have not ate yet. However, instead of first
proceeding to seg to promptly attend to those diabetics who are in acute
distress, nurses are instead choosing to administer insulin to the
diabetics in general population. Next, they are choosing to perform pill
call for the entire non-diabetic general population.
Depending on the efficiency of the particular nurses working on a given
day, by the time it’s all said and done nurses aren’t arriving in seg
with glucose meters & insulin until anywhere from 7-10 a.m. every
morning, sometimes even later. Delays are also occurring at lunchtime
& suppertime, even though nurses are already clocked in and on duty,
and so there is really no explanation apparent to justify these
additional delays. I kept a record of the delays between meals &
insulin, and the nurses responsible for the worst delays are Nurse
Williams, Nurse Deefe, Nurse Gilbert, Nurse Porter, and Nurse Mills.
To clear the air on how dangerous hours-long delays are, I am going to
quote to you from page 54 of Dr. Jorge E. Rodriguez’s book Diabetes
Solution, where he explains the dangers of high blood sugar, also
called hyperglycerin:
“Hyperglycemia, by definition, is a level of sugar in the blood above
the accepted normal range… the normal range for a person’s fasting blood
sugar (”fasting” means after 8 or more hours without eating anything)
level is below 100 milligrams per deciliter (mg/dl) of blood, and the
normal range at any other time should be below 180 mg/dl)… Elevated
blood sugar in and of itself causes tissue damage but having a blood
sugar that is extremely elevated can cause life-threatening changes in
the body in a matter of hours. An extremely high blood sugar level, and
I mean at least 300 – remember, normal is under 100 (fasting) or 180
(any other time) – can cause an imbalance in the delicate acid-based
structure in the tissues of the body. When the body can no longer use
sugar as an energy source it starts breaking down fat and protein, one
of the by-products of these two alternative sources of energy is
ketones. A high level of circulating ketones not only damages tissues,
but can cause confusion, unconsciousness, and coma.”
The above medical expert’s opinion sufficiently shows how diabetics
housed in CSP’s segregation unit are in imminent danger of serious
physical injury and/or death. Georgia Department of Corrections (GDC)
will try to remedy a prisoner’s medical complaints by transferring him
to another prison. In just 3 years my complaints of improper diabetic
care has caused my transfers to 8 different prisons (there is also a
deficiency in the diabetic care at my present prison, Wheeler
Correctional Facility).
These repeated failures are evidence which supports a civil complaint,
not only against these individual prisons, but against the entire GDC,
under the litigation theory that there’s no prison in the GDC network it
can transfer me to where I won’t be in imminent danger of serious
physical injury or death, due to a lack of adequate diabetic care. I
will keep you informed of all the latest developments.
MIM(Prisons) responds: This is a followup to the articles
“Insulin
Indifference Endangers Prisoners”, and
“Fixing
Insulin Indifference”, which we published in 2017 on this same
insulin problem in Georgia. These medical battles are literally life and
death for some people. Just a further example of the indifference and
negligence of the criminal injustice system.
The enclosed letter is submitted to you for follow-up to
“Insulin
Indifference Disables Prisoners”.(ULK 57, p. 6) The
publishing editor of that letter omitted the solution to that problem.
Does anyone have time to comment on if mine compares to the grievance
guides presently available? Or is my method in conflict with the advice
in other manuals? I want to know how I compare with other grievance
methods.
The problem in the article is a policy of no lunchtime
fingersticks/insulin injections. The prison serves lunch so late it is
outside the timeframe that a pre-breakfast shot of 70/30 insulin works
for some diabetics within the prison.
For diabetics having this problem, immediately following lunch they may
have symptoms of extremely elevated glucose, like hunger (even though
they have just ate lunch), blurry vision, dry mouth, thirst, pins and
needles (like tingling nerve pain), and frequent urination. In addition,
at next fingerstick before supper their glucose may be extremely
elevated.
“Extremely elevated” blood sugar is dangerous because it “can cause life
threatening changes in the body within a matter of hours. An extremely
high blood sugar level… And I am talking at least 300… can cause an
imbalance in the delicate acid-based structure in the tissues of the
body.”(1)
So if you take 70/30 insulin (and your prison doesn’t do lunchtime
fingersticks/insulin injections) and you have the above symptoms, and/or
if your suppertime glucose level is still over 300 several hours after
lunch, then you should first try a medical request. Then, if necessary,
a grievance explaining the problem. If filing a grievance (the formal
step), then include the illustration of how extremely elevated glucose
harms the body, located in the last paragraph of “Insulin Indifference
Disables Prisoners.” This way the warden, or other prison officials
signing off on the grievance, cannot claim they were unaware of the
damage that was occurring due to that they “are not medical
professionals.” (This is a popular excuse used by non-medical prison
officials to escape liability in prison medical care cases.)
Two solutions to the problem are: 1. For the prison to start serving
lunch earlier, or 2. For the prison to start providing lunchtime
fingerstick/insulin injection, at which time you should receive a small
dose of regular-type insulin, also called “mealtime insulin.”
Immediately following these two suggested solutions on your grievance,
you should write “To do neither would constitute deliberate
indifference.”
In your medical request or your grievance, you should also explain that
staff should periodically adjust your new lunchtime dose of regular
insulin to determine exactly what amount is required to lower the
residual glucose from lunch so it is at least somewhere between 200 -
300 by suppertime fingerstick. This will keep your glucose out of the
danger zone between lunch and supper.
MIM(Prisons) responds: The problem with timing insulin injections
with mealtimes is not lack of education or medical expertise. The
problem of indifference is built in to the capitalist, white supremacist
power structure. Imprisoned people, and oppressed nations in general,
are not thought to need or deserve to have access to proper medical
care. Prisoners’ right to their eyesight or to keep all their toes is of
absolutely no concern to the imperialist power structure. In fact, from
the imperialist system’s perspective it is probably better for prisoners
and oppressed nation people to continue suffering, and be kept busy
filing grievances. That way it’s even harder to fight back.
We’re glad this author wrote in with more details on what people could
do to resolve the individual problems they are having with
administration’s approach to diabetes management. If we’re talking about
real remedies, though, and about fixing a problem, we need to
acknowledge that capitalism and national oppression are the real cause
of extremely elevated glucose levels. We need to struggle on our
individual problems so we can be stronger for our revolutionary work.
Don’t lose sight of the bigger picture!
On 26 October 2017, U.$. President Trump declared the opioid epidemic a
public health emergency. The declaration should lead to more federal
funding for grants to combat opioid abuse.(1) As we explain below, this
epidemic disproportionately affects euro-Amerikans. Trump linked his
campaign to build a wall along the current Mexican border to the battle
against this epidemic, despite the fact that prescription painkillers
are at the root of it. This is consistent with the Amerikan government’s
solution for drug problems created by imperialism. For the crack
epidemic of the 1980s Amerika responded with mass incarceration of New
Afrikan men as the solution. As opioid addiction continues a steady
rise, Trump offers further militarization of the border.
Opioids have been used by humyns for thousands of years both medicinally
and recreationally, with many periods of epidemic addiction. Use began
with opium from poppies. Morphine was isolated in 1806. By the early
1900s heroin was promoted as a cure for morphine addiction in the United
$tates, before being made illegal in 1924. There was a lull in heroin
use during the 1980s, when cocaine and crack overshadowed it. Various
prescription pain killers began to come back into vogue in the 1990s
after the “Just Say No!” mentality was wearing off. Since then, use and
abuse has been on a steady rise, feeding a new surge in the use of
heroin as a cheaper alternative. This rise, in the economic centers of
both the United $tates and China, is directly linked to capitalism.
The Danger
While K2
is one dangerous substance plaguing U.$. prisons these days, partly
due to its undetectability, opioids are by far the biggest killer in the
United $tates, and we expect that is true in prisons as well. Drug
overdoses surpassed car accidents as the number one cause of accidental
deaths in the United $tates in 2007 and has continued a steady rise ever
since. The majority of these overdoses have been from opioids.(2)
While the increase in deaths from opioids has been strong across the
United $tates, rates are significantly higher among whites, and even
higher among First Nations. One reason that use rates are lower among
New Afrikans and Latin@s is that it has been shown that doctors are more
reluctant to prescribe opioids to them because they are viewed as more
likely to become addicted, and Amerikan doctors see them as having a
greater pain threshold.(3)
We did see some evidence of this trend in the results of
our
survey on the effects of drugs in U.$. prisons. The most popular
answer to our question of whether certain groups did more drugs in
prison than others was no, it affects everyone. But many clarified that
there was a strong racial divide where New Afrikans preferred weed and
K2, while whites and usually Latin@s went for heroin and/or meth. Some
of these respondents said that New Afrikans did less drugs.(4) A couple
said that New Afrikans used to do less drugs but now that’s changing as
addiction is spreading. In states where K2 has not hit yet (CA, GA, CO)
it was common to hear that whites and “hispanics” (or in California,
“southern” Mexicans) did more drugs. The pattern of New Afrikans
preferring weed and K2 seemed common across the country, and could have
implications for strategies combating drug use among New Afrikans
compared to other groups. In particular, stressing that K2 is completely
different and more dangerous than weed could be part of a harm reduction
strategy focused on New Afrikans.
If prison staff were doing their jobs, then we would expect rates of
both overdoses and use in general to be lower in prisons. But we know,
and our survey confirmed, that this is not the case (78% of respondents
mentioned staff being responsible for bringing in at least some of the
drugs in their prison). In hindsight, it may have been useful to ask our
readers what percentage of prisoners are users and addicts. Some of the
estimates that were offered of the numbers using drugs in general were
20-30%, 90%, 75%, and many saying it had its grips on the whole
population.
Deaths from opioids in the general U.$. population in 2015 was 10.5 per
100,000, double the rate in 2005.(5) This is higher than the rates in
many state prison systems for overdoses from any drug,
including Florida, Georgia, Illinois, Ohio, Texas and Pennsylvania that
all reported average rates of 1 per 100,000 from 2001-2012. California
was closer at 8 per 100,000 and Maryland exceeded the general population
at 17 deaths from overdoses per 100,000 prisoners.(6) At the same time,
prison staff have been known to
cover
up deaths from overdoses, so those 1 per 100,000 rates may be
falsified.
In our survey of ULK readers, we learned that Suboxone, a drug
used to treat opioid addiction, is quite popular in prisons
(particularly in the northeast/midwestern states). Survey respondents
mentioned it as often as weed as one of the most popular drugs, and more
than heroin. Suboxone is actually used to treat heroin addiction. And
while it is not supposed to be active like other opioids, it can lead to
a high and be addictive. It is relatively safe, and will not generally
lead to overdose until you combine it with other substances, which can
lead to death.
Prescription drugs are not as common as other drugs in most prisons,
according to our survey. Though in some cases they are available. We
received a few responses from prisons where prescription drugs
prescribed by the medical staff seemed to be the only thing going on the
black market. Clearly there is variability by facility.
Two Paths to Recovery
The increases in opioid abuse in the United $tates has been
staggering, and they cause a disproportionate amount of the deaths from
drug overdoses. About 10% of opioid addicts worldwide are in the United
$tates, despite only being less than 5% of the world’s population.(7) At
the same time, only about 1% of people in the United $tates are abusing
opioids.(8) This is not the worst episode in U.$. history, and certainly
not in world history.
Around 1914 there were 200,000 heroin addicts in the United $tates, or
2% of the population. In contrast, some numbers for opium addicts in
China prior to liberation put the addiction rate as high as 20% of the
population around 1900, and 10% by the 1930s. That’s not to dismiss the
seriousness of the problem in the United $tates, but to highlight the
power of proletarian dictatorship, which eliminated drug addiction about
3 years after liberation.
Richard Fortmann did a direct comparison of the United $tates in 1952
(which had 60,000 opioid addicts) and revolutionary China (which started
with millions in 1949).(9) Despite being the richest country in the
world, unscathed by the war, with an unparalleled health-care system,
addicts in the United $tates increased over the following two decades.
Whereas China, a horribly poor country coming out of decades of civil
war, with 100s of years of opium abuse plaguing its people, had
eliminated the problem by 1953.(9) Fortmann pointed to the politics
behind the Chinese success:
“If the average drug addiction expert in the United States were shown a
description of the treatment modalities used by the Chinese after 1949
in their anti-opium campaign, his/her probable response would be to say
that we are already doing these things in the United States, plus much
more. And s/he would be right.”(9)
About one third of addicts went cold turkey after the revolution, with
the more standard detox treatment taking 12 days to complete. How could
they be so successful so fast? What the above comparison is missing is
what happened in China in the greater social context. The Chinese were a
people in the process of liberating themselves, and becoming a new,
socialist people. The struggle to give up opium was just one aspect of a
nationwide movement to destroy remnants of the oppressive past.
Meanwhile the people were being called on and challenged in all sorts of
new ways to engage in building the new society. There was so much that
was more stimulating than opium to be doing with their time. Wimmin, who
took up opium addiction in large numbers after being forced into
prostitution in opium dens, were quickly gaining opportunities to engage
at all levels of society. The poor, isolated peasants were now organized
in collectives, working together to solve all kinds of problems related
to food production, biology and social organization. The successful
struggle against drug addiction in China was merely one impressive side
effect of the revolutionizing of the whole society.
In contrast, in the capitalist countries, despair lurks behind every
corner as someone struggles to stay clean. The approach has ranged from
criminalization to medicalization of drug addiction as a disease. “Once
an addict, always an addict”, as they say. Always an individualist
approach, ignoring the most important, social causes of the problem.
That drug addiction is primarily a social disease was proven by the
practice of the Chinese in the early 1950s, but Western “science”
largely does not acknowledge the unquestionable results from that
massive experiment.
It is also worth pointing out the correlation between drug abuse and
addiction, and capitalist economics specifically. Whether it was
colonial powers forcing opium on the Chinese masses who had nothing, in
order to enslave them to their economic will, or it is modern Amerikan
society indulging its alienation in the over-production of prescription
pills from big pharmaceutical companies marketing medicine for a profit.
China Today
And now, opioid addiction is on the rise again in capitalist China after
decades. A steady rise in drug-related arrests in China since 1990 are
one indicator of the growing problem.(10) As more profits flowed into
the country, so have more drugs, especially since the 1990s. We recently
published a
review
of Is China an Imperialist Country?, where we lamented the loses
suffered by the Chinese people since the counter-revolution in 1976. It
goes to show that when you imitate the imperialists, and put advancing
the productive forces and profits over serving the people, you invite in
all the social ills of imperialism.
In China drug addiction has now become something that people fear.
Like it did with its economy, China has followed in the imperialists’
footsteps in how it handles drug addiction. Chinese policy has begun
treating addicts as patients that need to be cured to protect society.
Rather than seeing those who give up drugs as having defeated the
oppressor’s ways, they are monitored by the state, lose social
credibility, and have a hard time getting a job.(11) Under socialism,
everyone had a job and no one needed recreational drugs to maintain
themselves mentally. The path to combating drug addiction and abuse is
well-established. Attempts under imperialism that don’t involve
liberatory politics of the oppressed have little to no effect.
6 September 2017 – I am writing this letter to inform you of the recent
adverse reactions of offenders to a new batch of a K2-styled substance.
About a month ago a new batch of “2uece”, “K2” or “tune” arrived on the
unit. I was in the prison chapel and overheard a conversation that 9
people that day had been taken away in an ambulance. A few days later I
saw 2 people fall out at work in the kitchen after smoking it. The user
will experience temporary paralysis, unable to move or even speak. Users
will watch their “friends” pass out, then laugh at their friends and
continue smoking the same K2. Another prisoner bragged to me of his
smoking prowess. He said, “I already had 3 people who smoked this shit
with me get stuck. They think they can smoke like me.” Later that day
after having that conversation, that offender collapsed, unconscious and
was rushed to medical. He may have died for all I know.
Then the next day as I was leaving the shower area, they shut down the
hallway for an emergency and they were carrying 2 paralyzed prisoners to
sickbay (medical). I personally have seen more than 20 people carried
away in stretchers this past month. I would estimate well over a hundred
people have been transported to the hospital due to this new K2. I
further estimate 1/2 the entire unit are users. About 80% of the people
I work with smoke. Unlike other products such as ice cream, that might
get contaminated with listeria and recalled, with this so-called “2uece”
there is no recall. People will continue to sell it and smoke it, and
there will be more adverse reactions. Shame on the local media for not
reporting this! Shame on TDCJ for not locking down the prison, instead
being more concerned with the Estelle Unit textile plant profits!
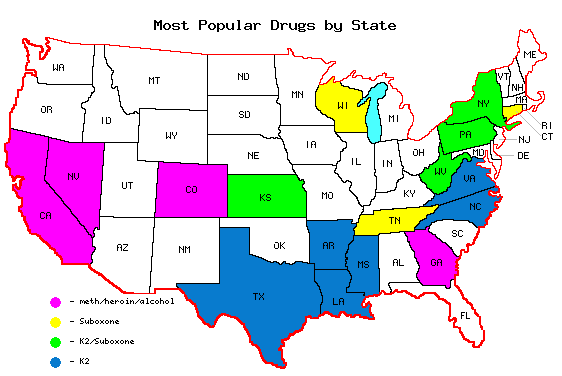
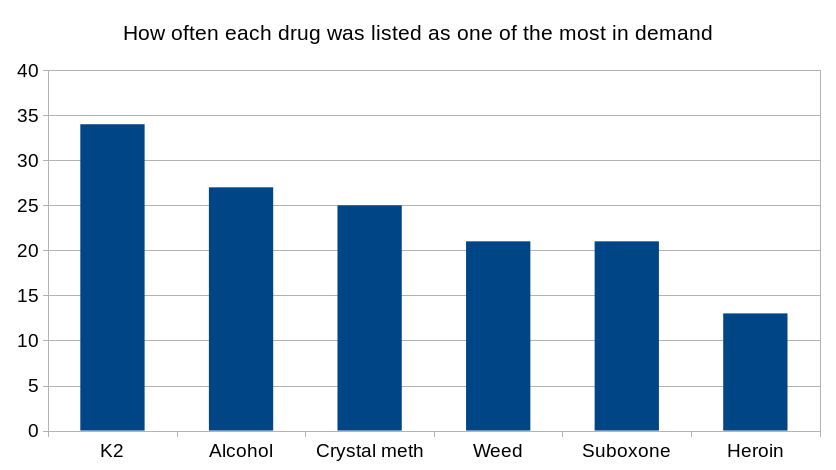
MIM(Prisons) responds: In our survey of ULK readers about
drugs in prison, K2 (Deuce, 2euce, Spice, or synthetic marijuana) stood
out as the most popular drug. While in the chart below, other drugs
aren’t too far behind in number of mentions, K2 was often highlighted as
the #1 choice, with one Texas prisoner stating that everything else
there is now irrelevant. Suboxone was the other one that really stood
out, because it was less familiar and being reported a lot. Suboxone is
actually used to treat drug addiction to opioids, but has more recently
proven to be addictive itself even though it does not have the same
effects on your body that opioids do.
The states of California, Nevada, Colorado and Georgia differed from the
rest of the states in not really mentioning K2 or Suboxone. Instead in
those states the combination of crystal meth (ice, sk8), heroin and
alcohol were popular.
Many of these drugs are a serious health risk, and we address opioids in
a separate article. However, K2 seems to deserve special attention right
now due to the prevalence and risk. The risk is partially due to the
variability in what you are getting when you purchase “K2”, as the
comrade alludes to above. While it is referred to as “synthetic weed”
because of the receptors in the brain that it acts on, it is very
different from weed with very different effects. In the prisons where it
was reported as easiest to get, our respondents reported death from
drugs at their prison 50% of the time. In contrast, the prisons where K2
was not listed among drugs easiest to get death was only reported 19% of
the time. This difference was statistically significant. While this
correlation does not establish a definitive link with K2 as the cause of
excess deaths, anecdotal responses like the reports above and below seem
to indicate that is the case. In the last two years, news stories about
group overdoses from bad batches of spice have become frequent. Our
correspondents talk about people being “stuck” when they are on K2. This
drug can be completely disabling and can lead directly to death.
The K2 epidemic is not limited to Estelle Unit, but is across the Texas
Department of Criminal Justice (TDCJ) system, where our respondents
consistently listed it as the most common drug. As the map above shows,
the problem extends to many other states.
A comrade in Larry Gist Unit in Texas reported on 14 September 2017:
“I want to file a lawsuit against the Sr. Warden and American
Correctional Association (ACA) who pass the Unit Larry Gist inspection
because the speaker communication do not work and about 7 to 10
prisoners died smoking K2 from heart attack and other sickness. Speaker
communication is very important and maybe if the speaker communication
had been working 1, 2 or 3 of the prisoners that died could have been
saved.”
A comrade at Telford Unit in Texas reported on 23 August 2017:
“My brothers in here have fallen victim to K2, which is highly
addictive. They don’t even care about the struggle. The only thing on
their minds is getting high and that sas. I mean this K2 shit is like
crack but worse. You have guys selling all their commissary, radios,
fans, etc. just to get high. And all these pigs do is sit back and
watch; this shit is crazy. But for the few of us who are K2-free I’m
trying to get together a group to help me with the struggle.”
We had a number of surveys filled out in Texas, all of which put the
majority, if not all of the blame for the drugs entering the TDCJ on
staff. Prisoners are a vulnerable population due to the degree of
control that the state has over their lives. The injustice system leads
to a disproportionate number of people in prison with substance abuse
histories. It is completely irresponsible and tragic that people are
then put in conditions where there is an epidemic of dangerous,
unregulated drugs when they enter prison.
Under a socialist society, where we have a system of dictatorship of the
proletariat, with those in power acting in the interests of the formerly
oppressed peoples, individuals responsible for mass deaths through
negligence or intentional actions will be brought to justice. Prison
administrators who help bring in drugs known to kill people need to face
the judgment of the people. These deaths are easily prevented.
In the meantime, we commend the comrades at Telford Unit who are
starting to organize support for people to stay out of this epidemic
that is affecting so many Texas prisoners. It is only by building
independent institutions of the oppressed, which serve the people, that
we can overcome this plague.
On 15 September 2017 my neighbor died smoking K2 and after the pigs saw
I was the last person to speak with him they locked me up under
investigation. The first interrogation was conducted by the Arkansas
state pig and it seemed as if all was well. The next week another death,
same cause. Then my neighbor’s mom appeared on the news saying she was
gonna get to the bottom of his death (apparently they told her he had a
heart attack), and bring a lawsuit before the court.
So when the internal affairs came and conduct their interrogation the
pressure had been put on ADC (Arkansas Department of Corrections) and
the woman resorts to some dirty ass tactics as soon as I walk in. She
starts by telling me she’s been doing her thorough investigation and
listening to my phone calls, and that she knows about my girlfriend that
I tell that I love her and then call my wife and turn around and tell
her the same. I ask her if it was some type of threat she was implying
because what she was talking about had nothing to do with my neighbor’s
death. She then starts her backpedaling and starts questioning me about
$ I had moved in the “free.” That’s where I decided to end our
conversation.
Right before the time period for investigation ran out I received a
disciplinary for possession of contraband even though I was never in
possession of anything and it was at this point I realized ADC had their
scapegoat in the form of myself. That week topped off with another
death, same cause. That’s 4 deaths from K2 in this prison within 90 days
(there was one about a month before my neighbor).
I was found guilty in kangaroo court, given 30 days punitive and 60 days
restriction on phone, visits, commissary. A few days later, the Arkansas
state pig comes back. The only reason I could see was to fish for some
more circumstantial evidence and bring some type of formal charges to
cover ADC’s ass. I’ve been in the hole for about 40 days now and as far
as that situation, that’s where things stand.
MIM(Prisons) adds: We just completed a survey
of drugs in U.S. prisons, in which we found K2 to be the new
dominant drug across much of the country. See our article on the
K2
epidemic in Texas, where a similar rash of deaths have occurred.
Drugs in prison is a sensitive topic in the convict world. Being that I
live in it and that I am STG’d out here in Arizona, I will refrain from
speaking/writing about the illegal kind as here in solitary they are not
as prevalent as they are out there on the yards. I will not lie though,
and say that they are non-existent here, as all convicts know “where
there is a will, there is a way.” But what I mean is that there is no
one all strung out or in debt and so forth.
The number one drug here is the pills that the contract medical
provider, Corizon Health, Inc., is giving to everyone, i.e. the legal
kind. These prescription drugs that come in the guise of treatment are
what reigns supreme here in SMU. You don’t even have to wait for visit
on the weekends like on the yard. No way not here, here they are passed
out on the daily, twice a day, even three times a day to some. These
drugs are prescribed by so called “clinicians who use an evidence based
approach to treat conditions such as yours which includes maximizing
formulary medication use while providing safe and effective treatment,”
to quote Corizon staff verbatim. This is actually impossible as you
cannot eyeball someone and use that as your evidence. That is just a
guess, and not an educated one.
Now that they have taken actual pain medication, which is only
gabapentin, a pill to treat nerve damage, Corizon staff have been
directed to prescribe psych drugs in replacement. So instead of further
treatment that include MRIs, EMG treatment, physical therapy, or a range
of other options, they are taking away a drug that works, to prescribe
you an anti-depressant for pain management as if the depression from you
being here was causing you pain and not the stenosis in your neck, AC
joint separation, nerve damage, etc. This psych med is like the
commercials that you see on TV where the side effect is diarrhea,
headache, etc.
The system gives you these legal drugs instead of approving further
treatment because MRIs cost money, and outside care visits cost money.
So they want you on psych meds to have you walking around like a zombie
or not so depressed from being STG’d and housed in solitary. Even the
law firms and organizations representing us in Parsons v. Ryan
are aware, yet choose to do nothing. Corizon staff and Arizona
Department of Corrections (ADC) staff actually tell you to seek outside
legal representation, like a dare! But while all we want is to be
treated for our injuries and not drugs, ADC will not step in nor will
our so-called legal team. Instead, our drugs at this unit are more
habit-forming and more highly accessible than the illegal kind, and will
continue to be supplied by our very own med provider Corizon, and all
legally.
ADC will just allow this to continue to take place and protect their
mule, Corizon, just like the drug cartels in the motherland. This is
ADC’s “plaza” and Corizon will continue to funnel drugs all over the
state of Arizona, not through tunnels, planes, boats, or on foot but
right through the front gate with a badge and a greeting, service with a
smile!
MIM(Prisons) responds: This writer brings up an important point
about drugs in prison. The problem isn’t just illegal drugs numbing
minds and harming bodies, it’s also legal drugs being prescribed by the
prison medical teams to keep the population pacified. This pacification
happens through the action of anti-depressants and anti-psychotics,
which can dull all emotions, and also through addictive drugs like pain
meds. Instead of treating the real problems, both physical and
emotional, that are caused by years of living in the harmful conditions
of Amerikan prisons, prison medical staff just treat the symptoms, if
they offer any treatment at all.
From the capitalist perspective, in the short term providing inadequate
health care and getting people addicted to pacifying drugs is an
effective way to control costs and control the prison population. But in
the long term this makes no sense, even for the capitalists. Health
problems left untreated will only get worse as people age, and become
more expensive to deal with. Further, releasing prisoners addicted to
pain killers or other drugs does not lead to productive life on the
streets.
This only makes sense in the context of a criminal injustice system that
wants to maintain a revolving door of an expanding prison population.
One that doesn’t care if prisoners live or die, as long as they stay
passive. While it may be true that cost is part of the reason good
treatment isn’t provided, Amerikans are happy to spend lots of money on
prisons in general. Spending all that money is justified because the
prisons provide an effective tool of social control, targeting oppressed
nations and all who resist the capitalist system. The drugs given to
prisoners behind bars are just one part of that control.







{kind=link}